
COMPREHENSIVE GUIDE TO MEDICAL MALPRACTICE DEFENCE IN INDIA: LEGAL FRAMEWORK, CASE LAW, AND PROFESSIONAL SUPPORT FOR HEALTHCARE PROFESSIONALS
Curated & Authored by
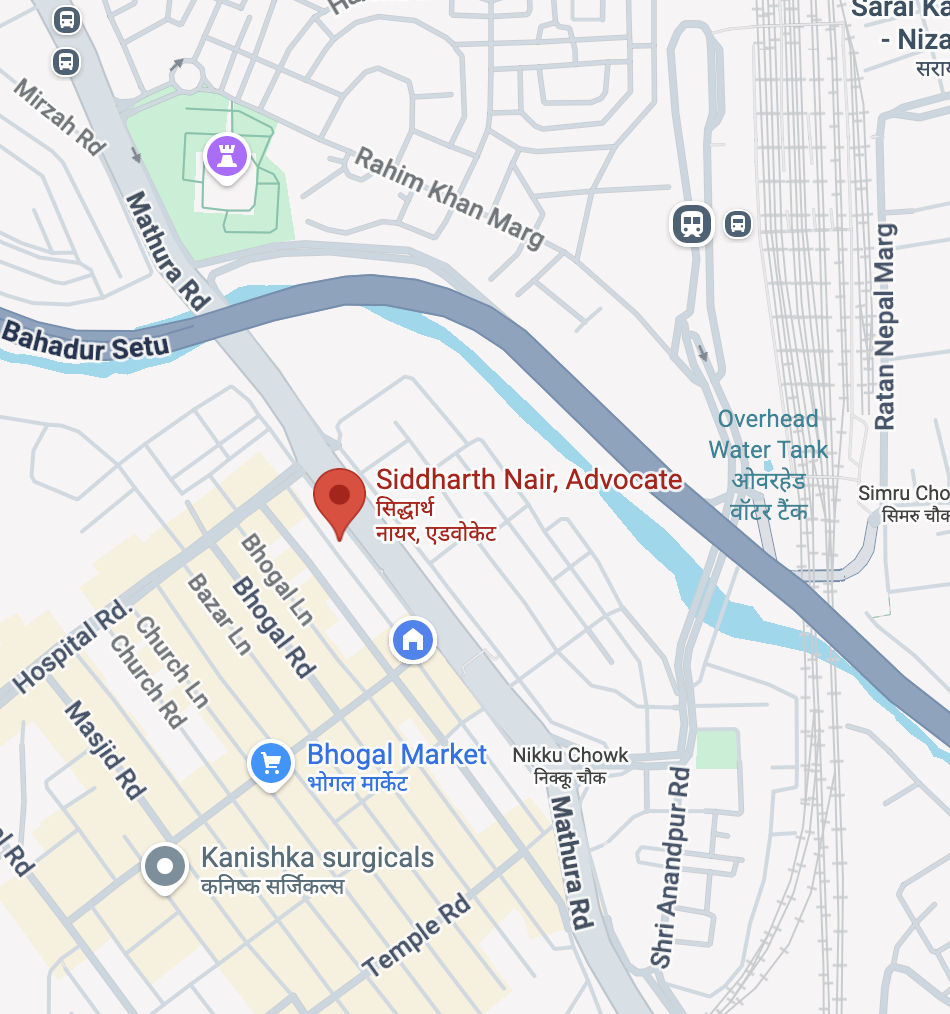
Advocate Siddharth Nair
Call: +91-9625799959
Leading Criminal Defence & Medical Malpractice Lawyer – New Delhi & Delhi NCR
Call, Text or Visit Now For Help!
At:
Office: 434, Lower Ground Floor, Jangpura, Mathura Road, New Delhi, NCT of Delhi, India-110014
Phone: +91-9625799959
Email: mailme@nairlawchamber.com
Website: www.nairlawchamber.com
PROFESSIONAL DEFENCE COUNSEL FOR MEDICAL MALPRACTICE CASES
Overview for Healthcare Professionals in India
Best Guide Medical Negligence Cases New Delhi
Healthcare professionals—including doctors, surgeons, anaesthetists, nurses, lab technicians, pharmacists, paramedics, and pharmaceutical companies—face increasingly complex legal challenges related to medical malpractice allegations in India. The Indian legal system distinguishes sharply between civil liability and criminal liability in medical negligence cases, with criminal prosecution requiring proof of “gross negligence” rather than simple medical errors.
A specialized criminal defence advocate experienced in medical malpractice cases serves as an essential guardian for healthcare professionals facing allegations. This comprehensive guide outlines the legislative framework, landmark judicial precedents, investigative procedures, and strategic defence mechanisms available to medical professionals navigating India’s intricate medico-legal landscape.
SECTION 1: COMPREHENSIVE LEGISLATIVE FRAMEWORK
Best Guide Medical Negligence Cases New Delhi
A. CRIMINAL LIABILITY PROVISIONS
1. Indian Penal Code (IPC), 1860 – Relevant Sections
Section 304A – Causing Death by Negligence
- Maximum punishment: 2 years imprisonment OR fine OR both
- Applies to death caused by rash or negligent act not amounting to culpable homicide
- Requires proof that negligence was “gross” and amounted to recklessness
- For medical professionals, requires deviation from standard medical practice
- Expert medical opinion mandatory before prosecution under this section
Section 106 – Bharatiya Nyaya Sanhita (BNS), 2023 (Replacement for 304A)
- Enhanced provision for death by negligence
- General negligence: up to 10 years imprisonment
- Medical professionals: Limited to maximum 2 years imprisonment
- Reflects legislative recognition of need for special protections for doctors
- Requires “gross negligence” and reckless conduct
- Medical Board opinion prerequisite before FIR registration
Section 336 – Act Endangering Life or Personal Safety
- Applies when negligent act does not cause hurt but endangers life
- Maximum punishment: 3 months imprisonment OR fine up to Rs. 250 OR both
- Relevant for diagnostic errors or treatment failures without injury
Section 337 – Causing Hurt by Rash or Negligent Act
- Applies when negligent act causes hurt to patient
- Maximum punishment: 6 months imprisonment OR fine up to Rs. 500 OR both
- Requires proof of causation between breach and injury
- Defence available if treatment was within standard medical practice
Section 338 – Causing Grievous Hurt by Rash or Negligent Act
- Applies when negligent act causes grievous hurt
- Maximum punishment: 2 years imprisonment OR fine up to Rs. 1,000 OR both
- Grievous hurt includes loss of limbs, vision, hearing, or disfigurement
- Requires demonstration of breach of duty of care
Section 52 – Act in Good Faith
- Critical protection for medical professionals
- Provides immunity if act done in good faith for benefit of person with consent
- Protects doctors performing emergency interventions
- Defence counsel should emphasize good faith and patient benefit
Section 80 – Accident in Doing Lawful Act
- Protects from liability if negligence committed while doing lawful act
- Applicable when error occurs during proper medical procedure
- Defence available if practitioner exercised reasonable care
Section 88 – Act Not Intended to Cause Death, Done by Consent
- Protects medical professionals acting with patient’s informed consent
- Requires good faith and reasonable belief that act will benefit patient
- Essential in surgical interventions and invasive procedures
- Emphasizes importance of documented informed consent
Sections 319-322 – Causing Hurt and Grievous Hurt
- Apply when injury occurs due to negligence
- Require proof of intention or knowledge
- Not typically applicable if negligence was inadvertent
- Defence based on absence of mens rea (criminal intent)
Section 201 – Destruction of Evidence
- Critical provision: Tampering with medical records attracts criminal liability
- Punishable with imprisonment up to 7 years
- Undermines defence credibility significantly
- Medical professionals must preserve all original records
Sections 340-342 – Wrongful Confinement
- Applicable in cases of unauthorized detention for non-payment
- Common allegation in private hospital contexts
- Defence available if confinement was medically justified
Section 491 – Breach of Contract
- Applies when medical service contract is breached
- Can result in charges under this section alongside negligence charges
- Requires proof of agreed-upon terms and breach
B. BHARATIYA NYAYA SANHITA (BNS), 2023 – KEY AMENDMENTS
Section 105 (Equivalent to Section 304)
- Culpable homicide punishments: up to life imprisonment
- Not applicable to medical professionals acting in good faith
Section 106 (Equivalent to Section 304A)
- “Causing Death by Act Endangering Life or Personal Safety”
- General punishment: imprisonment up to 10 years OR fine
- For medical professionals during treatment: Maximum 2 years imprisonment
- Represents legislative acknowledgment that doctors need differentiated protection
- Requires demonstration of acts “so rash or negligent as to manifest a depraved indifference to human life”
- Cannot be applied for errors of judgment if treatment was within accepted medical practice
Section 218 (Equivalent to Section 197 CrPC)
- Sanction requirement for prosecution of public servants
- Government medical professionals require government sanction
- Adds procedural protection for government doctors
- Private practitioners exempt from this sanction requirement
C. CONSUMER PROTECTION ACT, 2019
Scope of Medical Services
- Covers all medical services provided for remuneration
- Includes private hospitals, nursing homes, diagnostic centers, clinics
- Applies to both individual doctors and healthcare institutions
- Free medical services excluded from coverage
Section 2(1)(o) – Definition of Deficiency
- “Any shortfall or inadequacy in quality, nature, manner, characteristics or level of performance required to be maintained by service provider”
- Medical negligence falls within definition of deficiency
- Burden of proof: Preponderance of evidence (lower than criminal standard)
- Complainant must prove negligence more likely than not
Complaint Filing Timeline
- Must be filed within 2 years from date of injury (Section 69)
- Consumer defined broadly to include patients and legal heirs
- Can be filed by patient, family members, or legal representatives
Compensation Awards
- Not limited by statutory maximums in medical negligence cases
- Awards include: medical expenses, lost wages, pain and suffering, mental agony
- Interest: 8% per annum from date of complaint
- Costs and compensation for false claims possible
Remedies Available Under CPA
- Monetary compensation for harm suffered
- Compensation for mental agony and suffering
- Refund of medical fees
- Punitive damages (up to 3 times actual loss)
- Costs of litigation
- Orders to rectify deficiency
D. INDIAN MEDICAL COUNCIL ACT, 1956 / NATIONAL MEDICAL COMMISSION ACT, 2019
Professional Conduct Regulations
- Indian Medical Council (Professional Conduct, Etiquette, and Ethics) Regulations, 2002
- Now administered by National Medical Commission (NMC) established 2020
- Sets ethical standards for medical practitioners
- Violations can result in disciplinary action separate from criminal/civil proceedings
Grounds for Disciplinary Action
- Conviction in criminal court (triggers mandatory inquiry)
- Negligence or misconduct in professional practice
- Gross violations of ethical guidelines
- Improper advertising or touting for business
- Breach of patient confidentiality
- Incompetence or lack of necessary qualification
- Performing unnecessary procedures
- Failure to maintain medical records
- Violation of statutory requirements (Transplantation Act, PCPNDT Act, etc.)
Penalties by Medical Councils
- Suspension of registration (temporary or permanent)
- Cancellation of license to practice
- Reprimand or warning
- Monetary fine
- Mandatory training in specific areas
- Restrictions on specific procedures
Statute of Limitations
- No express limitation period for medical council proceedings
- Can be initiated by patient, police, court conviction, or suo moto
- Separate from civil and criminal proceedings
E. SPECIALIZED MEDICAL LEGISLATION
The Pre-Conception and Pre-Natal Diagnostic Techniques (Regulation and Prevention of Misuse) Act, 1994 (PC-PNDT Act)
- Prohibits sex-selective abortion
- Applies to gynecologists, ultrasound technicians, diagnostic centers
- First conviction: Imprisonment up to 3 years, fine up to Rs. 10,000
- Second conviction: Imprisonment up to 5 years, fine up to Rs. 1,00,000
- Medical professional can lose license for violation
The Bharatiya Nyaya Sanhita, 2023 – Sections on Abortion
- Section 87: Emergency treatment in good faith—protected
- Section 88: Acts done by consent for person’s benefit—protected
- Critical for obstetric cases and gynecological emergencies
Transplantation of Human Organs Act, 1994
- Regulates organ transplantation procedures
- Violations can result in prosecution under IPC
- Medical professionals performing unauthorized transplants subject to imprisonment and fine
Drugs and Cosmetics Act, 1940
- Applies to drug administration and prescription
- Violations can be charged alongside medical negligence
- Pharmacists and doctors administering expired/substandard drugs liable
The Information Technology Act, 2000
- Relevant for telemedicine cases and electronic health records
- Applies to online medical consultations
- Cybersecurity and data privacy requirements
The Bharatiya Nyaya Sanhita, 2023 – Telemedicine Provisions
- Section 23: Medical advice through electronic means
- Same standards of care apply as in-person consultation
- Treatment over telephone/video must meet accepted standards

SECTION 2: LANDMARK SUPREME COURT CASES ESTABLISHING MEDICAL NEGLIGENCE STANDARDS
1. Indian Medical Association v. V.P. Shantha (1995) 6 SCC 651
Significance: Landmark judgment bringing medical services within Consumer Protection Act
Facts:
- Question whether medical practitioners render “service” under CPA
- Whether healthcare falls within definition of consumer transaction
Key Holdings:
- Medical services constitute “service” under CPA 2019
- Patients are “consumers” capable of filing complaints under CPA
- Bolam Test applied: Doctor not negligent if endorsed by responsible body of medical opinion
- Medical practitioners must exercise skill and care of reasonably competent doctor in similar circumstances
- Standard of care determined by practices accepted among medical community
Legal Principles Established:
- Negligence = Failure to exercise reasonable skill and care in medical practice
- Adoption of Bolam Test from English law: “act as an ordinarily competent professional”
- Difference in medical opinion between doctors not evidence of negligence
- Doctor protected if practice endorsed by responsible medical opinion
Application to Defence Counsel Strategy:
- Obtain affidavits from senior doctors supporting treatment approach
- Demonstrate that chosen treatment falls within accepted medical practice
- Show that multiple schools of thought exist on treatment methodology
- Establish that responsible body of medical opinion supports defendant’s approach
2. Jacob Mathew v. State of Punjab (2005) 6 SCC 1
Significance: Landmark judgment establishing threshold for criminal prosecution of doctors; defines “gross negligence” requirement
Facts:
- Dr. Jacob Mathew charged under Section 304A IPC for patient’s death
- Patient allegedly denied oxygen due to empty cylinder
- Complaint lodged by patient’s son alleging criminal negligence
- Trial court framed charges; doctor challenged prosecution
Key Holdings:
- Criminal negligence must be “gross” – mere error of judgment insufficient
- Negligence must demonstrate “gross dereliction of duty” or “reckless conduct”
- Must show “gross lack of competence, inaction, and wanton indifference to patient safety”
- Degree of negligence required for criminal liability higher than civil liability
- Doctor’s conduct must manifest “depraved indifference to human life”
- Hospital management negligence (empty oxygen) distinct from doctor’s conduct
Guidelines Established by Supreme Court:
- Private complaint requirement: Prima facie evidence of gross negligence required before magistrate entertains complaint
- Medical Board examination: Investigating officer should obtain independent medical opinion before proceeding
- Bolam Test application: Whether conduct endorsed by responsible body of medical opinion
- Arrest prohibition: Doctor should not be arrested unless necessary for investigation
- Good faith protection: Doctors acting in good faith protected from frivolous prosecution
- Expert opinion mandatory: Court proceedings must be based on credible medical expert opinion
Critical Distinction:
- Civil negligence: Failure to exercise reasonable care (lower threshold)
- Criminal negligence: Gross negligence amounting to recklessness (higher threshold)
Application to Defence Counsel Strategy:
- Challenge FIR registration without independent expert medical opinion
- File petition under Section 482 CrPC to quash proceedings without proper expert evaluation
- Seek quashing at threshold if allegations, even accepted as true, do not constitute gross negligence
- Emphasize distinction between medical error and criminal behavior
- Obtain expert affidavits establishing that treatment was reasonable under circumstances
3. Kusum Sharma v. Batra Hospital and Medical Research Centre (2010) 3 SCC 480
Significance: Comprehensive guidelines on medical negligence; establishes duty of care framework
Facts:
- Patient died following pancreatic surgery and treatment
- Alleged negligence in diagnosis, surgical technique, and post-operative care
- Complaint filed under Consumer Protection Act
- Hospital challenged findings and sought damages limitation
Key Holdings:
- Three-Part Test for Medical Negligence:
- Doctor owed duty of care to patient
- Breach of that duty occurred
- Breach resulted in causally connected injury/death
- Standard of Care Definition:
- “Reasonably skilled medical professional would have adopted”
- Not highest standard, but ordinary standard for that specialty
- Account taken for experience level and qualifications of doctor
- Burden of Proof:
- Complainant must prove negligence on preponderance of evidence
- Cannot presume negligence from bad outcome
- Requires expert opinion supporting negligence allegations
- Causation Requirement:
- Breach must be probable cause of injury, not merely possible cause
- If multiple possible causes exist, must establish breach was most probable
- Expert Opinion Standards:
- Opinion must come from competent, impartial expert
- Expert must have relevant specialization
- Opinion must be based on accepted medical principles
- Mere difference of opinion insufficient to prove negligence
- Compensation Framework:
- Medical expenses for treatment and recovery
- Lost income during incapacity
- Pain, suffering, and mental agony
- Long-term care costs if applicable
Application to Defence Counsel Strategy:
- Ensure expert affidavits from practitioners in same specialty
- Establish that treatment choice falls within accepted practice spectrum
- Demonstrate that causation link is weak or speculative
- Show multiple possible causes for adverse outcome
- Emphasize that mere bad outcome not equivalent to negligence
4. Martin F. D’Souza v. Mohd. Ishfaq (2009) 3 SCC 1
Significance: Clarifies distinction between civil and criminal negligence standards
Facts:
- Accused charged with causing death by negligence under IPC 304A
- Court analyzed evidence standards for civil vs. criminal liability
Key Holdings:
- Different standards apply: Civil negligence ≠ Criminal negligence
- Civil: Failure to exercise reasonable care sufficient
- Criminal: Gross negligence or recklessness required
- Court cannot elevate civil negligence to criminal by mere terminology
- Jury/Court cannot upgrade negligence degree without factual basis
- Error of judgment alone never constitutes criminal negligence
Judgment Impact:
- Sets precedent limiting criminal prosecutions for medical errors
- Protects doctors from criminalization of judgment differences
- Emphasizes high burden of proof for criminal liability
Application to Defence Counsel Strategy:
- Argue that even if civil negligence exists, criminal threshold not met
- Distinction critical in cases where treatment choice differs from alternative methods
- Use to oppose framing of charges and secure acquittal or reduced liability
5. V. Kishan Rao v. Nikhil Super Speciality Hospital (2010) 6 BCR 155 SC
Significance: Addresses post-operative complications and medical negligence
Facts:
- Patient developed complications after surgery
- Complainant alleged negligent treatment post-operation
- Question whether doctor liability extends to all post-operative complications
Key Holdings:
- Known complications arising despite proper care not negligence
- Doctor not liable for complications occurring despite standard treatment
- Skill and competence judged by standards at time of treatment
- Risk disclosure in informed consent important but not determinative
- Post-operative complications within known risk spectrum not evidence of negligence
Application to Defence Counsel Strategy:
- Obtain literature establishing known complications of procedure
- Show risk was disclosed in informed consent
- Demonstrate standard care protocols were followed
- Use expert opinion to establish complication within expected range
6. Jacob Mathew v. State of Punjab (2005) – Further Clarifications on Gross Negligence
Extended Principle – “No Criminalization of Errors”:
- Medical professional must show “disdain for human life” for criminal liability
- Simple inadvertence or insufficient care = civil liability only
- Negligence must be of degree showing apathy toward patient safety
Critical Quote from Judgment:
“Where a patient’s death results merely from error of judgment or an accident, no criminal liability should be attached to it. Mere inadvertence or some degree of want of adequate care and caution might create civil liability but would not suffice to hold a doctor criminally liable.”
SECTION 3: HIGH COURT LANDMARK DECISIONS BY JURISDICTION
A. DELHI HIGH COURT
1. Shiv Kumar v. National Medical Commission, 2024 SCC OnLine Del 9059 (Decided 20-12-2024)
Facts:
- Petitioner’s wife admitted with severe diarrhea and complications
- Multiple hospitals involved in treatment
- Death after cardiac arrest and complications
- Alleged negligence in: ICU availability, timely investigations, medication dosage, discharge circumstances
Key Holdings:
- Court cannot review substantive conclusions of expert bodies (Medical Council) on judicial review
- Expert bodies (NMC/Medical Council) have primary responsibility for upholding medical standards
- Mere dissatisfaction with treatment outcome not sufficient for negligence finding
- Court must show deference to collective expert opinion
- Procedural deficiencies can be cured in appellate proceedings
- “Medical negligence is not established by mere dissatisfaction or assertion of ‘expected’ standard of care”
Significance:
- Emphasizes limited scope of judicial review in medical negligence cases
- Protects expert determinations from casual second-guessing
- Shows courts will uphold expert bodies’ findings if reasoned and thorough
Application to Defence Strategy:
- Obtain thorough medical council opinion
- Ensure expert body procedures are properly followed
- Demonstrate reasoned analysis by expert committees
- Use this case to resist judicial re-evaluation of expert findings
B. KERALA HIGH COURT
1. Dr. Joseph John v. State of Kerala, 2025 SCC OnLine Ker 3334 (Decided 19-05-2025)
Facts:
- Gastroenterologist treated kidney transplant patient over telephone
- Patient developed complications at midnight; doctor advised medication from home
- Patient died within hours
- Allegation: Failure to arrange physical examination; reliance on phone consultation
Key Holdings:
- “Not every death during treatment warrants criminal prosecution”
- Criminal liability attaches only for “gross lack of competence or inaction and wanton indifference”
- Phone consultation not inherently negligent if appropriate under circumstances
- Unexpected medical deterioration at night not attributable to doctor’s negligence
- Expert panel opinion that treatment appropriate protects from criminal prosecution
- Proceedings constitute abuse of process without concrete evidence of gross negligence
Critical Quote:
“Even where a patient’s death results from an error of judgment or an unforeseen accident, such circumstances do not automatically attract criminal liability. Mere inadvertence or a certain degree of insufficient care might give rise to civil liability, but would not, by itself, be sufficient to hold a medical professional criminally liable under the law.”
Significance:
- Shows Kerala HC’s protective stance toward medical professionals
- Demonstrates that phone/remote consultation can be appropriate in certain contexts
- Emphasizes requirement for concrete evidence of gross negligence
Application to Defence Strategy:
- Establish that remote consultation or advice was reasonable given circumstances
- Show patient was under appropriate monitoring by other specialists
- Obtain expert opinions supporting the consultation method used
2. Kerala High Court – Guidelines for Medical Negligence Cases (2025)
12-Point Draft Guidelines Issued:
- Expert Panel constitution within 30 days of requisition
- Prima facie material required before charges
- Written representations from both parties required
- Panel conclusion within 30 days
- In-person hearing if prima facie gross negligence found
- Findings must be specific about individual responsibility
- Cannot hold doctor liable on vicarious basis without direct evidence
- Consideration of emergency circumstances and clinical discretion
- Post-mortem analysis critical for causation determination
- Delays and complications do not automatically establish negligence
- Conservative management decisions protected if within medical practice
- Police not to register FIR without expert panel opinion
C. UTTAR PRADESH HIGH COURT
1. B.P. Mishra v. State of U.P., PIL No. 53904 of 2016 (Decided 14-11-2019)
Facts:
- Petitioner’s son admitted with viral fever diagnosis
- Medical test showed dengue symptoms not recognized by treating doctor
- Patient transferred in critical condition; died at higher center
- Clear diagnostic negligence by local doctor
Key Holdings:
- Gross medical negligence established when test results ignored
- Transparency in medical care obligatory—test findings must be acted upon
- Compensation proportional to severity of negligence
- State/hospital failures trigger regulatory action
- Courts can direct systemic improvements in healthcare facilities
Award:
- Compensation: Rs. 25 lakhs
- Directed to establish separate blood units for dengue patients
- Court ordered strict implementation of vector-borne disease regulations
Application to Defence Strategy:
- Ensure test results are reviewed and documented
- Act upon abnormal findings promptly
- Maintain transparent communication with patients
- Document clinical reasoning for treatment decisions
D. RAJASTHAN HIGH COURT
1. Rajasthan High Court – Vasundhara Hospital Case (2025)
Facts:
- Woman admitted for minor fibroid surgery; died post-operatively
- Alleged negligence: Inadequate pre-operative testing, delayed neurological evaluation
- Expert committee found no prima facie evidence of culpable negligence
- Court examined whether complications = negligence
Key Holdings:
- “Doctors have no incentive to willfully endanger life in trust-driven healthcare”
- Independent expert committee opinion critical
- Absence of historical evidence of negligence significant
- Medical complications alone insufficient without gross recklessness
- Surgical discretion protected even if outcome unfavorable
- Doctrine of ‘respondeat superior’ does not apply criminally without direct evidence
Court’s Reasoning:
- Treating doctors acted within clinical discretion during evolving emergency
- Cannot expect retrospective perfection in emergency situations
- Sepsis and MODS (Multi-Organ Dysfunction) known complications despite proper care
- Absence of complete records not grounds for presuming negligence
Significance:
- Shows Rajasthan HC’s protective approach toward medical professionals
- Requires concrete evidence of gross negligence, not speculation
- Recognizes emergency medical decision-making constraints
2. Rajasthan High Court – Anaesthetist Case (2025)
Facts:
- Anaesthetist posing as gynecologist; child died during delivery
- Unqualified person conducting medical procedure
- Clear case of fraudulent practice and negligence
Key Holdings:
- Fraudulent misrepresentation of qualifications establishes criminal liability
- Lack of technical expertise in critical procedures negligence per se
- Institutional failure to verify credentials constitutes negligence
- FIR maintainable when qualification fraud evidenced
Distinction:
- Court distinguished between qualified doctor error (protected) vs. unqualified fraud (criminal)
E. MADHYA PRADESH HIGH COURT
1. Dr. B.C. Jain v. Maulana Saleem (MP High Court Judgment)
Significance: Issued comprehensive guidelines for government doctors facing negligence prosecution
Guidelines Established:
- Medical Board Constitution:
- Minimum 3-doctor board required
- Constituted by Dean of Government Medical College
- Must occur within 7 days of requisition
- Doctor’s Right to Reply:
- Written response required to allegations
- In-person hearing available upon request
- Board must record reasoned findings
- Timeline Requirement:
- Board proceedings must conclude within 60 days
- Expedited timeline protects accused from prolonged uncertainty
- FIR Registration Restriction:
- No FIR without Medical Board opinion
- FIR only if Board finds prima facie gross negligence
- Police must conduct preliminary inquiry first
- Sanction Requirement:
- If Board finds gross negligence, sanction required under Section 197 CrPC
- Government has 30 days to grant/refuse sanction
- Court cannot proceed without sanction for government doctors
- Complaint Case Procedure:
- Complaint under Section 200 CrPC cannot proceed without Board opinion
- Court cannot take cognizance under Section 156(3) CrPC without Board report
- Civil vs. Criminal Distinction:
- Mere civil negligence insufficient for criminal proceedings
- Board must opine on criminal (gross) negligence specifically
Application to Defence Strategy:
- Strictly comply with Medical Board procedures in MP
- File written response emphasizing reasonable care taken
- Request in-person hearing to explain clinical decision-making
- Obtain supporting expert opinions for Board consideration
- Challenge FIR if registration preceded Board opinion
F. PUNJAB & HARYANA HIGH COURT
1. Failed Surgery Case – Medical Negligence Cannot Be Presumed
Key Holding:
- “Medical negligence cannot be presumed solely based on the unsuccessful outcome of a surgery”
- Absence of allegations questioning surgeon’s competence = no negligence claim
- Surgeon entitled to attempt procedure if qualifications present
- Adverse outcome ≠ negligence
Application to Defence:
- Emphasize surgeon’s qualifications and experience
- Show that adverse outcome falls within known surgical risks
- Establish that alternative approach might not have succeeded either
2. Max Hospital – Pacemaker Case (Gross Medical Negligence Found)
Key Holding:
- Installing substandard/cheap device without disclosure = gross negligence
- Deception regarding materials used = criminal conduct
- Amounted to “cheating” in addition to negligence
Distinction:
- Court upheld proceeding where misrepresentation occurred
- Doctor liable for fraudulent practice, not mere medical error
G. MADRAS (TAMIL NADU) HIGH COURT
1. K. Mubeena Banu v. Tamil Nadu Health & Family Welfare Department, 2023 SCC OnLine Mad 3951
Facts:
- Mother petitioned for compensation for child with cardiac abnormality
- Alleged inadequate treatment and refusal to provide advanced care
- Sought damages via writ petition
Key Holdings:
- Writ petition not appropriate forum for medical negligence claims
- High Court cannot examine medical expertise or act as medical expert
- Medical negligence cases require specific forums (Consumer Court, Civil Court)
- Government hospitals entitled to provide treatment within available resources
- Discrimination in treatment among patients violates Article 21
- But cannot expect more than reasonably available resources provide
Critical Principle:
- Court will not interfere with speciality medical decisions
- Trial-natured proceedings (medical evidence evaluation) improper in writ jurisdiction
Application to Defence:
- Cite proper forum requirements to dismiss inappropriate petitions
- Establish that government hospitals provide reasonable care with available resources
H. WEST BENGAL HIGH COURT
1. Commission under West Bengal Clinical Establishments Act v. Appellant (Supreme Court Review), 2025
Facts:
- Patient received care from unqualified personnel (echocardiography technician)
- Discharge summary misrepresented patient condition as “stable” when precarious
- Commission directed compensation; High Court questioned jurisdiction
Supreme Court Holding:
- Commission’s power to grant compensation distinct from Medical Council’s power
- Both can operate in parallel without one excluding the other
- Commission examines “deficiency in service”; Council examines “negligence”
- Medical council proceedings not prerequisite for commission jurisdiction
Application to Defence:
- Understand parallel proceedings can occur
- Prepare defenses for multiple forums simultaneously
2. West Bengal – Nursing Home Death Case (2024-2025)
Facts:
- Woman died post-delivery without doctor attendance
- Nursing home liable for gross negligence and abandonment
Key Holding:
- Failure to provide doctor presence for post-delivery monitoring = gross negligence
- Compensation: Rs. 2-10 lakhs depending on detailed findings
- Medical Council found doctor guilty of professional negligence
Application to Defence:
- Ensure appropriate medical coverage for post-operative/post-delivery care
- Document presence and monitoring of critical patients
I. BOMBAY HIGH COURT / GOA
1. Dr. Dilip Amonkar v. State of Goa (2023)
Facts:
- Senior government surgeon alleged negligent in appendectomy treatment
- Patient developed complications post-op, transferred to another hospital
- Allegation of inadequate pre-operative testing and documentation
Key Holdings:
- Bolam Test applied: Doctor not negligent if conduct endorsed by responsible medical opinion
- Pre-operative testing not negligent if decision within doctor’s discretion
- Senior doctor entitled to rely on clinical judgment
- Transfer to higher center appropriate when complications develop
- Conduct unbecoming of profession (not reviewing consent) noted but not grounds for criminal conviction
Critical Distinction:
- Findings of misconduct (disciplinary) vs. criminal negligence separate
- Medical Council can discipline for conduct unbecoming while courts acquit of criminal charges
Award:
- Criminal charges dismissed
- Medical Council issued reprimand for conduct issues
Application to Defence Strategy:
- Distinguish between disciplinary misconduct and criminal negligence
- Show respect for patient autonomy even if documentation flawed
- Obtain expert support for clinical decisions made
SECTION 4: INVESTIGATIVE AGENCIES AND REGULATORY BODIES
A. PRIMARY INVESTIGATIVE AGENCIES
1. Police (Criminal Investigation Department / Local Police)
- Role: Registers FIR under Section 154 CrPC following medical negligence complaint
- Investigation Lead: Inspector/Sub-Inspector conducts preliminary inquiry
- Authority Source: IPC/BNS and CrPC/BNSS
- Timeline: Usually 90 days for investigation completion
- Key Requirement: Medical Board opinion must precede FIR (per Jacob Mathew guidelines and MP/Kerala HC orders)
- Arrest Authority: Cannot arrest without proper justification or necessity
- Evidence Collection: Medical records, witness statements, expert opinions
2. Forensic Medicine/Medical Board (State/District Level)
- Constitution: 3+ doctors from government medical colleges
- Role: Examination of medical records and facts to opine on gross negligence
- Timeline: 30-60 days for completion (per NMC guidelines)
- Authority: Can conduct independent examination, interview parties
- Opinion Scope: Prima facie evidence of gross negligence only
- Use of Opinion: Prerequisite for FIR registration in many states
3. District Medical Board
- Composition: District-level expert panel
- Jurisdiction: Initial review of negligence allegations
- Timeline: 30-45 days typically
- Authority: Can recommend to state-level board if complex
- Appeal Avenue: Higher board review available
4. State-Level Apex Medical Expert Committee
- Composition: Senior doctors from various specialties
- Jurisdiction: Appeal against district board findings
- Authority: Final opinion on prima facie gross negligence
- Timeline: 30-60 days from appeal receipt
- Binding Effect: Police must follow opinion for FIR registration
B. REGULATORY AND PROFESSIONAL BODIES
1. National Medical Commission (NMC)
- Established: 2020 (replaced Medical Council of India)
- Authority: Under National Medical Commission Act, 2019
- Jurisdiction: National-level regulation and discipline
- Powers:
- Maintain national medical register
- Establish professional conduct standards
- Conduct disciplinary proceedings
- Suspend or cancel medical licenses
- Issue guidelines for investigation of negligence
- Complaint Procedures:
- Complainants file with State Medical Council
- Council investigates and reports to NMC
- NMC Board examines findings
- Appeal to NMC President if dissatisfied
- Timelines:
- Preliminary inquiry: 30 days
- Full investigation: 60 days typically
- Final decision: 90-180 days from complaint receipt
- Recent Guidelines (2024):
- Mandated 2-week preliminary assessment
- Earlier timelines throughout
- Direct appeal to state board (skipping divisional board)
2. State Medical Councils
- Role: Primary professional regulator at state level
- Jurisdiction: All registered medical practitioners in state
- Authority: Investigate complaints, hold disciplinary hearings, impose penalties
- Powers:
- Temporary suspension of registration
- Permanent cancellation of license
- Reprimand or warning
- Mandatory training orders
- Monetary fines
- Complaint Sources:
- Public complaints
- Police complaints
- Court referrals
- Suo moto actions
- Procedural Protections:
- Doctor entitled to notice of charges
- Opportunity to file written reply
- Right to hearing and cross-examination
- Appeal to appellate authority
- Appeal to NMC
- Timelines:
- Acknowledgment of complaint: Within 7 days
- Preliminary inquiry: 30 days
- Show cause notice: After preliminary inquiry
- Formal hearing: Within 60 days of show cause
- Final order: Within 30 days of hearing
3. Consumer Protection Authorities
District Consumer Disputes Redressal Commission
- Jurisdiction: Claims up to Rs. 50 lakhs
- Forum: 3-member panel (President + 2 members)
- Authority: Hear complaints under CPA 2019
- Timeline: Typically 12-24 months from complaint to final order
- Remedy: Compensation, interest, costs, penalties
State Consumer Disputes Redressal Commission
- Jurisdiction:
- Claims between Rs. 50 lakhs and Rs. 2 crore
- Appeals from district commission
- Forum: 3-5 member panel
- Timeline: 18-36 months typically
- Appeal Path: To NCDRC
National Consumer Disputes Redressal Commission (NCDRC)
- Jurisdiction: Claims above Rs. 2 crore (or Rs. 1 crore if specific public interest involved)
- Forum: 5-7 member bench
- Authority: Appellate and original jurisdiction
- Timeline: 24-48 months typically
- Final Authority: Appellate review with limited grounds
C. GOVERNMENT OVERSIGHT AGENCIES
1. District Magistrate (Civil Administration)
- Role: Can intervene in cases involving public hospitals or government doctors
- Authority: Can direct inquiries, impose administrative sanctions
- Powers: Can constitute independent committees
- Jurisdiction: Public health and safety within district
2. Health Department (State/National)
- Role: Regulatory oversight of hospitals and practitioners
- Authority: Can direct investigations, implement safety measures
- Powers: Hospital accreditation, facility inspection, compliance monitoring
3. Directorate of Medical Education
- Role: Oversight of government medical colleges and attached hospitals
- Authority: Can direct investigations, impose disciplinary measures
- Functions: Medical Board constitution, expert committee oversight
D. INVESTIGATIVE PROCEDURE TIMELINE
Phase 1: Preliminary Inquiry (0-30 days)
- Complaint received by police/medical council
- Initial statements from parties and witnesses
- Medical records obtained
- Police decision on FIR registration
Phase 2: Medical Board Opinion (30-60 days)
- Board constitution by competent authority
- Document review by board members
- Personal hearing with accused (if requested)
- Board report on prima facie gross negligence
Phase 3: FIR Registration (60-90 days)
- Based on medical board opinion (if supported)
- Section 154 CrPC First Information Report registered
- Notification to accused
- Investigation period begins
Phase 4: Investigation (90-180 days)
- Collection of evidence
- Expert witnesses identified
- Medical literature review
- Charge sheet preparation
Phase 5: Prosecution/Complaint Case (180+ days)
- Charge sheet filed or complaint case instituted
- Cognizance taken by court
- Summons/warrant issued
- Trial commencement
SECTION 5: LEGAL CHALLENGES FACED BY HEALTHCARE PROFESSIONALS
A. PROCEDURAL CHALLENGES
1. Frivolous and Vexatious Complaints
- Medical professionals frequently targeted with complaints lacking merit
- Challenge: Overcoming presumptions against medical professionals in public consciousness
- Defence Strategy: Early intervention at FIR stage; petition for quashing under Section 482 CrPC
- Time Cost: 6-12 months minimum to quash meritless FIR
2. Multiple Concurrent Proceedings
- Same case pursued simultaneously in: Criminal court, Consumer forum, Medical council
- Each forum has different burdens of proof and standards
- Defence Challenge: Coordinating defense across multiple jurisdictions with different rules
- Resource Cost: Requires separate counsel in each forum; multiple defense strategies
3. Arrest Despite Jacob Mathew Guidelines
- Despite Supreme Court guidelines against arrest, doctors still arrested
- Challenge: Securing anticipatory bail or bail after arrest
- Time to Bail: 2-4 weeks minimum; expensive process
- Damage: Reputation loss, embarrassment, media coverage
4. Delayed Prosecution Despite Weak Evidence
- Cases languish for years without resolution
- Challenge: Career uncertainty, professional limitations, continuous legal stress
- Time Frame: 3-10 years for acquittal in meritless cases
- Psychological Impact: Severe stress, financial burden, professional development stoppage
B. SUBSTANTIVE LEGAL CHALLENGES
1. Expert Opinion Deficiencies
- Medical Board opinions often lack specificity or thoroughness
- Challenge: Opinions sometimes not rooted in accepted medical practice
- Defence Strategy: Challenge expert credentials, methodology, and assumptions
- Counter: Obtain better quality affidavits from renowned specialists
2. Burden of Proof Confusion
- Public and sometimes judges conflate civil and criminal burdens
- Challenge: Educating courts about “beyond reasonable doubt” vs. “preponderance”
- Defence Strategy: Continuous emphasis on higher criminal threshold
- Impact: Requires persistent legal education of courts
3. Causation Proof Complexity
- Medical causation often multifactorial
- Challenge: Proving breach did NOT cause injury among multiple possible causes
- Defence Strategy: Medical literature showing alternative causation paths
- Expert Input: Causation specialists critical
4. Informed Consent Disputes
- Patients claim no consent obtained or risks not disclosed
- Challenge: Lack of proper written consent documentation
- Defence Strategy: Contemporaneous records; witness testimony
- Prevention: Digital consent systems with time-stamp verification
C. SOCIETAL AND PERCEPTION CHALLENGES
1. Anti-Medical Professional Sentiment
- Public perception: “All doctors are profit-driven negligent practitioners”
- Media Coverage: Negative stories amplified; acquittals under-reported
- Challenge: Defending against public prejudice in cases with media attention
- Impact: Jury perception (where applicable) prejudiced
- Defence Strategy: Media counter-narrative; expert commentary; public education
2. Power Imbalance
- Patients/families often economically weaker
- Public sympathy naturally flows to “victim” family
- Challenge: Courts sometimes overcorrect in favor of patients
- Impact: Judges may apply lower evidentiary standards
- Defence Strategy: Emphasize rule of law; transcend sympathy with evidence
3. Class-Based Litigation
- Private hospital doctors more sued than government doctors
- Perception: Private doctors prioritize profit over care
- Challenge: Overcoming class bias in litigation
- Defence Strategy: Distinguish between profit and professionalism
4. Medical Malpractice “Crisis” Narrative
- Media portrays epidemic of medical negligence
- Challenge: Assumption of guilt in some cases
- Impact: Difficulty securing unbiased judicial consideration
- Defence Strategy: Statistical evidence of actual negligence rates
SECTION 6: TIME DURATION FOR CASE RESOLUTION
A. TYPICAL CRIMINAL CASE TIMELINE
FIR to Acquittal – Average Duration: 5-15 Years
Breakdown:
Phase 1: FIR to Cognizance (0-6 months)
- Complaint filing: 1 week – 1 month
- Preliminary inquiry: 1-3 months
- Medical Board opinion: 1-2 months
- FIR registration: 3-6 months total
Phase 2: Investigation (6-18 months)
- Evidence collection: 2-3 months
- Expert opinions: 2-3 months
- Chargesheet preparation: 1-2 months
- Total: 6-18 months (often extends to 2 years)
Phase 3: Trial Initiation (18-30 months)
- Summons/Warrant issuance: 1 month
- Appearances/Pleas: 1-3 months
- Charge framing: 1-2 months
- Total: 3-6 months from FIR to chargesheet filing
Phase 4: Trial Proceedings (30 months – 10+ years)
- Witness examination: Highly variable
- Expert evidence: 6-12 months (often)
- Defense case: 6-18 months
- Arguments and judgment: 6-12 months
- Total trial time: 1-8 years
Phase 5: Acquittal/Conviction (10-15+ years)
- First court verdict: 10-15 years from FIR
- If appeals: Add 2-5 more years per appeal level
Factors Extending Duration:
- Court Congestion: India has 45+ million pending cases; average case takes 4-7 years
- Expert Witness Unavailability: Doctors reluctant to testify; frequent adjournments
- Medical Complexity: Cases requiring extensive expert evidence take longer
- Appeal Layers: District Court → High Court → Supreme Court (each 2-3 years minimum)
- Sanction Delays: Government sanction under Section 197 CrPC can delay 6+ months
B. CIVIL LITIGATION TIMELINE (CONSUMER COURT)
Complaint to Compensation – Average Duration: 2-5 Years
- District forum: 12-24 months
- State commission appeal: 12-24 months
- NCDRC final hearing: 12-36 months
- Total: 2-5 years (sometimes 7+ years)
C. MEDICAL COUNCIL DISCIPLINARY PROCEEDINGS
Complaint to Final Decision – Average Duration: 6-24 Months
- Preliminary inquiry: 1-3 months
- Show cause notice: 1 month
- Hearing: 1-2 months
- Judgment: 1-3 months
- Appeal to NMC: 6-12 months additional
- Total: 6-18 months for first-level decision; 12-24 months with appeal
SECTION 7: HOW A SPECIALIZED CRIMINAL DEFENCE ADVOCATE ASSISTS HEALTHCARE PROFESSIONALS
A. CASE ASSESSMENT AND STRATEGY
1. Immediate Case Evaluation
Upon engagement, a specialized medical malpractice defence counsel provides:
- Comprehensive factual analysis: Understanding all clinical decisions, timing, and patient progression
- Literature review: Establishing accepted medical practices in the specific clinical scenario
- Expert consultation: Preliminary discussion with senior physicians in relevant specialty
- Burden of proof analysis: Explaining criminal vs. civil standards to client
- Jurisdiction analysis: Identifying all potential forums (criminal, civil, medical council)
- Risk assessment: Realistic evaluation of prosecution likelihood and exposure
2. Preventive Legal Advice
Before prosecution initiates:
- Record preservation: Ensuring original medical records protected from tampering
- Witness identification: Identifying doctors, nurses, staff who observed treatment
- Expert engagement: Securing affidavits from senior specialists supporting treatment
- Document organization: Creating chronological medical narrative
- Media management: Advising on public statements and media interaction
B. INTERVENTION AT INVESTIGATION STAGE
1. Preliminary Inquiry Intervention
- Petition against FIR registration (Section 482 CrPC / Section 228 BNSS): If investigation initiated without requisite medical board opinion
- Representation before investigating officer: Providing expert opinion and detailed explanation of clinical decision-making
- Medical Board representation: Preparing comprehensive written submissions for medical board
- Witness coordination: Coaching medical witnesses for board examination
- Documentation submission: Providing medical literature supporting treatment approach
2. Section 197 CrPC Sanction Requirements (for government medical officers)
- Sanction necessity advice: Whether prior government sanction required
- Government liaison: Assisting in obtaining necessary government sanction
- Delay utilization: Using sanction period for additional investigation and case building
- Sanction refusal handling: If refused, pursuing quashing petition
C. FIR-STAGE INTERVENTIONS
1. Petition for FIR Quashing (Section 482 CrPC)
Filed when:
- FIR registered without medical board opinion
- Medical board opinion contradicts allegations
- Allegations, even if true, don’t constitute criminal negligence
- Gross negligence standard not met even prima facie
Drafting Strategy:
- Detailed factual narrative from medical records
- Expert opinions supporting treatment adequacy
- Case law emphasizing gross negligence requirement
- Causation analysis showing no nexus between breach and injury
Success Rate: 30-40% of medical negligence quashing petitions succeed in high courts
Timeline: 4-8 months from petition filing to decision
D. ARREST AND BAIL INTERVENTIONS
1. Anticipatory Bail
Sought before arrest to:
- Remain free during investigation
- Continue professional practice
- Facilitate legal preparation
- Avoid judicial custody trauma
Bail Conditions Negotiation:
- Frequency of police reporting (weekly vs. daily)
- Professional practice continuation permission
- Passport/travel restrictions
- Requirement to furnish sureties
2. Regular Bail (after arrest)
If arrested despite precautions:
- Immediate bail application filing
- Bail arguments emphasizing: Serious professional standing, roots in community, non-flight risk, cooperation with investigation
- Expert affidavits demonstrating case weakness
- Legal precedents on bail in medical negligence cases
Timeline to Bail: 2-4 weeks minimum; sometimes urgent hearings within 2-3 days
E. TRIAL-STAGE ASSISTANCE
1. Witness Preparation
- Medical witness coaching: Training for court testimony without appearing evasive or defensive
- Expert witness coordination: Briefing senior specialists on case facts and legal issues
- Cross-examination preparation: Preparation for aggressive questioning by prosecution/complainant counsel
2. Expert Evidence Procurement
- Affidavit drafting: Detailed affidavits from senior physicians supporting defendant’s approach
- Expert recruitment: Identifying renowned specialists willing to testify
- Literature compilation: Medical journals and textbooks supporting treatment choice
- Causation evidence: Establishing alternative causes for patient harm
- Standard of care documentation: Showing treatment within accepted practice
3. Defence Case Construction
Key Defence Arguments:
- Good faith treatment: Actions taken in patient’s best interest with care
- Standard of care compliance: Treatment fell within accepted medical practice
- Informed consent: Proper consent obtained with risk disclosure
- Causation absence: Breach did not cause alleged injury/death
- Alternative causation: Other factors caused patient harm (pre-existing condition, patient non-compliance, etc.)
- Expert support: Responsible body of medical opinion endorses treatment
- Error vs. negligence: Difference in outcome from error of judgment, not negligence
4. Cross-Examination of Prosecution Witnesses
- Expert opinion challenge: Questioning expert credentials, methodology, bias
- Causation challenge: Establishing speculative nature of cause-effect arguments
- Medical literature: Using published studies to contradict prosecution expert
- Alternative explanations: Presenting to prosecution expert and seeking acknowledgment
F. SETTLEMENT AND NEGOTIATION
1. Out-of-Court Settlement Negotiation
In civil and consumer forums:
- Early negotiation: Assessing settlement value and negotiating with complainant
- Mediation: Pursuing mediation before consumer forums (cheaper, faster)
- Partial settlement: Negotiating hospital/insurance company contributions vs. personal liability
- Confidentiality: Structuring settlements with confidentiality clauses
2. Plea Bargaining (Criminal cases)
Rarely applicable in medical negligence but:
- In multi-accused cases: Individual plea negotiations possible
- Charge reduction: Negotiating from 304A to 337 (lesser charge) if evidence weak
- Sentence negotiation: If conviction likely, negotiating lighter sentence
G. APPELLATE PRACTICE
1. High Court Appeals
Against acquittal or conviction:
- Grounds for challenge: Misapplication of law, perverse findings, procedural irregularities
- New evidence: Presentation of evidence not available at trial
- Bail pending appeal: Securing liberty during appellate proceedings
- Record scrutiny: Detailed analysis of trial court judgment for errors
2. Supreme Court Petitions
- Constitutional issues: Articles 21, 14 (right to life, equality)
- Legal precedent: Novel legal principles requiring apex court clarification
- Gross miscarriage: Severe procedural violations or patent injustice
SECTION 8: ASSISTANCE FOR VICTIMS OF MEDICAL MALPRACTICE
While this profile focuses on defending healthcare professionals, it’s important to recognize that genuine medical victims also require legal assistance. A comprehensive legal counsel familiar with medical malpractice law serves victims through:
A. VICTIM’S LEGAL RECOURSE
1. Criminal Complaint Filing
- Right to file FIR under Section 154 CrPC for gross negligence causing injury/death
- Requirement: Medical expert opinion establishing prima facie gross negligence
- Forums: Local police station or through public interest litigation
- Counsel role: Drafting detailed complaint with medical evidence and expert opinions
2. Civil Suit for Damages
- Right to sue for compensation under tort law
- Burden of proof: Preponderance of evidence (lower than criminal standard)
- Forums: Civil courts (District Judge or Additional District Judge)
- Counsel role: Evidence gathering, expert opinion procurement, damages calculation, trial representation
3. Consumer Court Complaint
- Right to file under Consumer Protection Act 2019
- Three-tier system: District → State → National Commission
- Burden of proof: Preponderance of evidence
- Advantages: Faster, lower filing fees, lower evidentiary burden than civil courts
- Counsel role: Complaint drafting, evidence management, representation at hearings
4. Medical Council Complaint
- Right to file with State Medical Council and National Medical Commission
- Process: Disciplinary inquiry into professional misconduct
- Remedies: Suspension/cancellation of license, reprimand, mandatory training
- Counsel role: Complaint preparation, evidence submission, representation at hearings
- Advantage: Can result in license cancellation protecting public from future harm
5. Additional Recourse Options
- Inspection of healthcare facilities: Right to file complaint with health department for facility inspection
- Regulatory complaints: Complaint to private healthcare regulator for facility non-compliance
- Insurance claims: Claim against healthcare provider’s professional indemnity insurance
- Compensation by National Consumer Disputes Redressal Commission: Compensation up to and exceeding Rs. 11 crores in egregious cases
B. VICTIM SUPPORT AND COMPENSATION FRAMEWORK
A compassionate advocate recognizes victim distress and assists:
1. Evidence Preservation
- Medical records compilation
- Witness statements collection
- Photography of injuries/complications
- Timeline documentation
2. Expert Opinion Procurement
- Engagement of independent medical experts
- Causation analysis by experts
- Deviation-from-standard-care evaluation
- Damages assessment (lost earnings, treatment costs, pain/suffering)
3. Compensation Calculation
- Medical treatment expenses (past and future)
- Lost income during recovery period
- Pain and suffering quantification
- Permanent disability assessment
- Long-term care cost projection
- Emotional trauma compensation
4. Victim Counseling
- Explanation of legal options and timelines
- Realistic assessment of compensation likelihood
- Emotional support during proceedings
- Guidance on managing stress during litigation
5. Institutional Accountability
- Ensuring hospital regulatory compliance
- Institutional reforms where systemic failures identified
- Public interest litigation for patient protection
- Recommendation for facility improvements
SECTION 9: DEFENCE COUNSEL STRATEGIC APPROACHES
A. JACOB MATHEW STRATEGY – THRESHOLD QUASHING
Applicable When: Allegations, even if wholly accepted, don’t constitute criminal negligence
Process:
- File petition under Section 482 CrPC in High Court
- Challenge FIR registration as against law
- Argue allegations don’t satisfy gross negligence threshold
- Cite Jacob Mathew standard: “Gross dereliction of duty” or “reckless conduct”
Success Factors:
- Detailed factual analysis showing reasonable care taken
- Expert affidavits supporting treatment appropriateness
- Medical literature citations
- Case law on gross negligence standard
Timeline: 3-6 months
Success Rate: 20-40%
B. MEDICAL BOARD OPINION STRATEGY
Applicable When: FIR registered without proper medical board opinion
Process:
- Petition High Court challenging FIR without board opinion
- Cite Madhya Pradesh HC guidelines requiring mandatory board opinion
- Request quashing based on procedural violation
- Alternative: Obtain independent board opinion supporting defense
Timing: Must be raised early in prosecution
Success Rate: 50-60% if procedural requirement clearly established in jurisdiction
C. CAUSATION CHALLENGE STRATEGY
Applicable When: Multiple possible causes for patient harm exist
Medical Literature Approach:
- Compile research showing injury/death possible despite proper treatment
- Show pre-existing conditions complicated outcome
- Establish patient non-compliance contributed to harm
- Present alternative medical causes
Expert Evidence:
- Obtain affidavits from senior physicians
- Show causation speculation by prosecution
- Highlight that breach was not probable cause
Success Rate: 30-50% depending on factual circumstances
D. INFORMED CONSENT STRATEGY
Applicable When: Patient claims no consent or inadequate risk disclosure
Documentation Approach:
- Obtain original consent form with patient signature
- Show date/time and patient’s full understanding
- Contemporaneous medical records of discussion
- Witness testimony from attendants present
Procedural Alternative:
- If consent form missing: Establish customs of consent through hospital procedure documentation
- Obtain institutional affidavits on standard consent practices
Expert Support:
- Expert affidavits on customary risk disclosure standards
- Literature on risks typically disclosed for procedure
Success Rate: 40-60% if contemporaneous documentation exists
SECTION 10: LEGISLATIVE PROTECTIONS FOR HEALTHCARE PROFESSIONALS
A. GOOD FAITH PROTECTIONS
Section 52 IPC: Act in Good Faith
- Protects doctors performing medical procedures in good faith
- Requirement: Belief that act will benefit person
- Consent (express or implied) required
- Protection extends to unforeseen but unavoidable consequences
Section 80 IPC: Accident in Doing Lawful Act
- Protects against liability for accident while performing lawful medical act
- Requirement: Act done without criminal rashness or negligence
Section 88 IPC: Act by Consent for Person’s Benefit
- Protects medical treatment with informed consent
- Requirement: Doctor reasonably believes treatment benefits patient
- Protection applies even if treatment fails or complications arise
Application:
- These sections should be prominently invoked in defense
- Good faith and benefit intention central to defense
- Consent documentation critical
B. JACOB MATHEW PROTECTIVE GUIDELINES
Now Statutory in Many States:
- No private complaint entertained without credible expert opinion
- Medical board opinion must precede FIR in many jurisdictions
- Arrest only if necessary for investigation
- Gross negligence standard applied consistently
- Courts should protect doctors from frivolous prosecution
C. SPECIALIZED PROTECTIONS FOR SPECIFIC PROFESSIONALS
Government Doctors (Section 197 CrPC):
- Prior government sanction required before prosecution
- Sanction process adds procedural layer
- Government incentivized to refuse sanction for weak cases
Emergency Medical Care Providers:
- Protected for acts in emergency if reasonable care taken
- Telemedicine practitioners: Same standard of care applies
- Remote consultation protected if appropriate under circumstances
SECTION 11: CASE PREPARATION CHECKLIST FOR DEFENCE ADVOCATE
Pre-Trial Preparation:
- Obtain complete patient medical records
- Compile relevant medical literature and guidelines
- Identify and consult potential expert witnesses
- Obtain affidavits from senior practitioners in specialty
- Review expert opinions filed by prosecution
- Identify procedural violations (if any) in investigation
- Prepare factual chronology of treatment events
- Document patient’s pre-existing conditions
- Gather hospital protocols and standard procedures followed
- Prepare detailed written submissions for court
- Draft potential cross-examination questions
- Identify alternative causation scenarios
- Compile institutional policies on consent, records management
- Prepare defendant for court testimony
Documentation Requirements:
- Original medical records with dates/times
- Consent forms signed by patient
- Prescription records and medication administration
- Nursing notes and vital sign documentation
- Investigation reports and findings
- Medical literature supporting treatment choice
- Expert affidavits (minimum 2-3 from reputed practitioners)
- Hospital/institutional procedures and protocols
- Witness statements from attending staff
- Communication records with patient/family
SECTION 12: CONCLUSION AND PROFESSIONAL ADVOCACY
Medical professionals in India face an increasingly litigious environment where even reasonable medical decisions can result in criminal prosecution. The distinction between criminal and civil liability remains poorly understood by many, leading to criminalization of medical errors.
A specialized criminal defence advocate serves as essential guardian of healthcare professionals’ rights by:
- Ensuring proper application of gross negligence standard: Protecting doctors from false criminalization
- Navigating complex legal and regulatory frameworks: Coordinating defense across multiple forums
- Procuring quality expert evidence: Demonstrating treatment appropriateness through medical literature and expert opinion
- Securing procedural protections: Invoking Jacob Mathew guidelines and statutory safeguards
- Obtaining favorable outcomes: Securing quashing of FIRs, acquittals, or minimal sanctions
The field of medical malpractice defence requires specialized knowledge of:
- Medical science and standards of practice
- Criminal and civil law principles
- Consumer protection jurisprudence
- Medical council regulatory procedures
- Contemporary judicial trends in medical negligence cases
Healthcare professionals accused of medical negligence should engage specialized counsel immediately upon receiving notice of complaint or investigation, as early intervention often prevents FIR registration through proper expert opinion and procedural compliance.
APPENDIX: KEY LEGAL CONTACTS AND FORUMS IN INDIA
Supreme Court of India
- Address: Tilak Marg, New Delhi 110001
- Medical Negligence Bench: Rotating benches
- Timeline: 2-3 years for hearing after petition filing
National Medical Commission (NMC)
- Address: New Delhi
- Jurisdiction: National-level professional regulation
- Complaint: Via State Medical Council
Consumer Forums
- District Consumer Commission: Claims up to Rs. 50 lakhs
- State Consumer Commission: Claims Rs. 50 lakhs to Rs. 2 crore
- NCDRC: Claims above Rs. 2 crore
State Medical Councils
- Each state has separate council
- Register with relevant state council for jurisdiction and procedures
Police Authorities
- Local police station for FIR registration
- CID for investigations
- District Magistrate for coordination
Click Here For MEDICAL MALPRACTICE DEFENCE & COMPLIANCE FRAMEWORK
CONTACT NOW:
AUTHOR & PRACTICE
Advocate Siddharth Nair
Criminal Defence & Medical Malpractice Lawyer
New Delhi | Delhi NCR | Pan-India
Advocate Siddharth Nair
Criminal Defence & Medical Malpractice Lawyer
Place: New Delhi | Delhi NCR | Pan-India
Office: 434, Lower Ground Floor, Jangpura, Mathura Road, New Delhi, NCT of Delhi, India-110014
Phone: +91-9625799959
Email: mailme@nairlawchamber.com
Website: www.nairlawchamber.com
DISCLAIMER
This document provides general legal information and educational guidance. It does not constitute legal advice for any specific case. Healthcare professionals facing medical negligence allegations should engage qualified criminal defence counsel familiar with medical law for specific guidance applicable to their circumstances. Legal outcomes vary based on jurisdiction, factual circumstances, quality of evidence, and judicial approach. This guide reflects legal principles as of December 2025 and should be updated with latest judicial pronouncements and legislative amendments.
Document Prepared: December 2025
Jurisdiction Coverage: Pan-India (with specific focus on Delhi, Kerala, Uttar Pradesh, Rajasthan, Madhya Pradesh, Punjab & Haryana, Tamil Nadu, Maharashtra, West Bengal, and Goa)
Legal Standard: Bharatiya Nyaya Sanhita 2023 and Consumer Protection Act 2019
©2026 www.nairlawchamber.com
1 thought on “Best Guide Medical Negligence Cases New Delhi”
Comments are closed.