New Delhi | Delhi NCR | Pan-India Jurisdiction
Advocate Siddharth Nair
Call: +91-9625799959
Leading Criminal Defence & Medical Malpractice Lawyer – New Delhi & Delhi NCR
Call, Text or Visit Now For Help!
At:
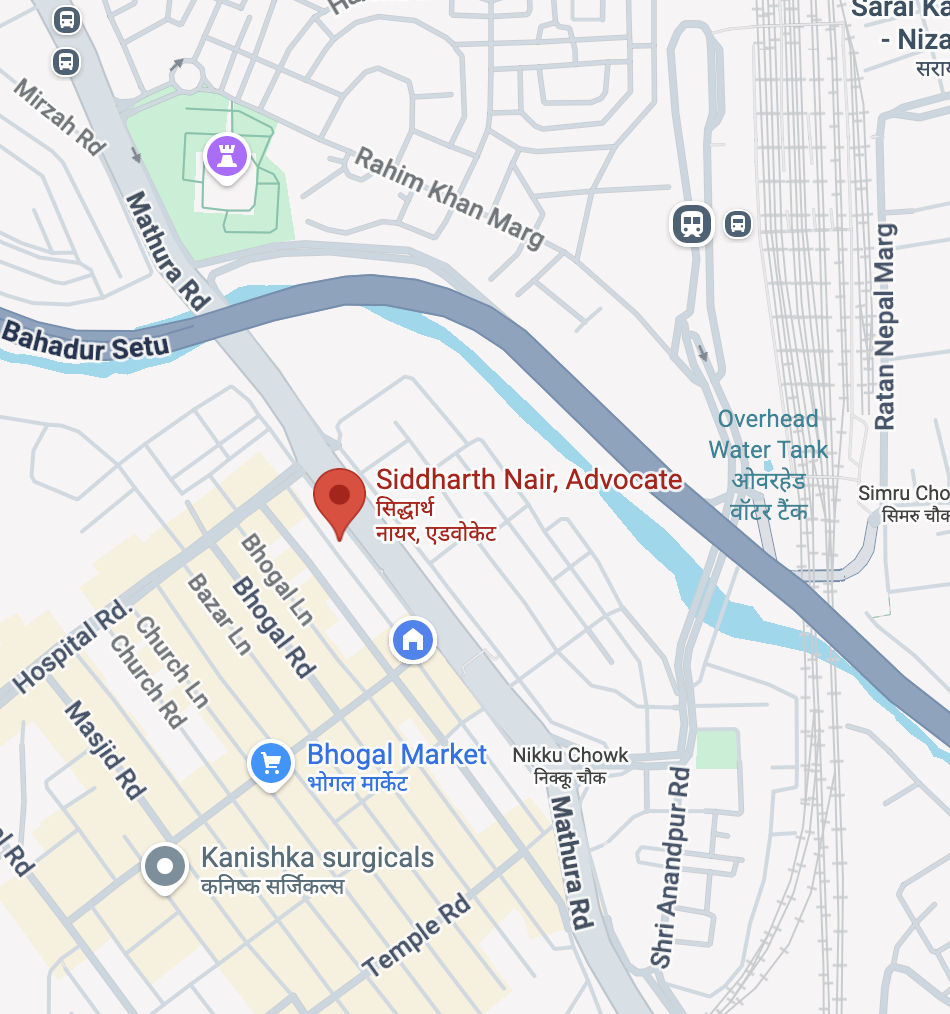
Office: 434, Lower Ground Floor, Jangpura, Mathura Road, New Delhi, NCT of Delhi, India-110014
Phone: +91-9625799959
Email: mailme@nairlawchamber.com
Website: www.nairlawchamber.com
Professional Overview: A Dedicated Criminal Defence Practice for the Medical Profession
Top Lawyer Medical Malpractice New Delhi & NCR
Advocate Siddharth Nair is a New Delhi–based criminal defence lawyer whose practice is exclusively distinguished by its focus on medical malpractice, healthcare prosecutions, and medico-legal criminal liability. His work spans trial courts, High Courts, and the Supreme Court of India, representing healthcare professionals and institutions facing criminal allegations arising out of medical treatment, procedures, pharmaceutical usage, diagnostics, and hospital administration.
In a legal ecosystem where medical outcomes are increasingly judged through a criminal lens, Advocate Siddharth Nair has built a practice grounded in the constitutional principle that criminal law must not punish professional judgment, scientific uncertainty, or therapeutic risk.
His role is not merely that of a defence lawyer, but of a strategic legal firewall between medical science and criminal prosecution.
2. Understanding Criminal Medical Malpractice in India: A Jurisprudential Context
Top Lawyer Medical Malpractice New Delhi & NCR
Indian courts have repeatedly recognised that:
- Medicine is not an exact science
- Adverse outcomes do not automatically imply negligence
- Criminal prosecution requires gross, reckless, or culpable negligence, not mere error of judgment
Despite this settled law, medical professionals in India frequently face:
- Immediate FIRs after patient deaths
- Arrest threats without expert opinion
- Parallel proceedings before police, medical councils, and consumer forums
- Media trials that prejudice investigations
Advocate Siddharth Nair’s practice is structured to restore the legal balance envisioned by the Supreme Court, ensuring that doctors are not converted into criminal accused for performing inherently risky professional duties.
3. Classes of Clients & Nature of Criminal Exposure
A. Individual Medical Professionals
- Physicians & super-specialists
- Surgeons (general, orthopaedic, cardiac, neuro, cosmetic)
- Anaesthetists & critical care doctors
- Obstetricians & gynaecologists
- Paediatricians & neonatologists
- Radiologists & pathologists
- Emergency medicine practitioners
- Resident doctors & interns
- Nurses, ward staff & paramedics
- Lab technicians & imaging personnel
Each professional category attracts distinct standards of care, decision-making autonomy, and vicarious exposure, which are central to defence strategy.
B. Institutional & Corporate Healthcare Clients
- Multi-speciality hospitals
- Private clinics & nursing homes
- Diagnostic laboratories
- IVF & fertility centres
- Blood banks
- Pharmaceutical companies
- Medical device manufacturers
- Clinical trial sponsors & CROs
For institutions, Advocate Siddharth Nair handles corporate criminal liability, including allegations of systemic negligence, protocol failure, understaffing, infrastructure deficiencies, and managerial culpability.
4. Comprehensive Legal Framework Governing Medical Malpractice Prosecutions
A. Indian Penal Code, 1860 (IPC)
(For acts prior to BNS enforcement)
Key sections frequently invoked:
- Section 304A IPC – Causing death by negligence
- Section 337 IPC – Causing hurt by negligent act
- Section 338 IPC – Causing grievous hurt by negligent act
- Section 268 IPC – Public nuisance
- Section 269 IPC – Negligent act likely to spread infection
- Section 270 IPC – Malignant act likely to spread infection
- Section 201 IPC – Disappearance of evidence
- Section 193 IPC – False evidence / falsification of records
- Section 120B IPC – Criminal conspiracy
- Section 34 IPC – Common intention
Advocate Siddharth Nair’s defence consistently demonstrates how mens rea and causation are absent in most medical prosecutions.
B. Bharatiya Nyaya Sanhita, 2023 (BNS)
For post-enactment offences:
- Re-codified negligence provisions
- Broader definitions of collective liability
- Increased emphasis on procedural compliance
Early interpretation and strategic use of transitional jurisprudence is a key feature of his advisory work.
C. Criminal Procedure Safeguards
Code of Criminal Procedure, 1973 / Bharatiya Nagarik Suraksha Sanhita, 2023
Critical provisions include:
- Section 41 & 41A CrPC – Protection from arbitrary arrest
- Section 154 CrPC – FIR registration standards
- Section 156(3) CrPC – Magistrate-directed investigation
- Section 173 CrPC – Police final report
- Section 227 & 239 CrPC – Discharge
- Section 482 CrPC – Quashing of FIR & proceedings
A significant percentage of cases handled by Advocate Siddharth Nair are terminated at the pre-trial or discharge stage, sparing clients prolonged litigation.
D. Consumer Protection Act, 2019 (CPA)
- Parallel civil liability
- Findings often misused in criminal cases
- Hospital vicarious liability
- Product liability against pharma & device companies
E. National Medical Commission Act, 2019 (NMC Act)
- Professional misconduct proceedings
- Ethics committee inquiries
- Suspension / cancellation of registration
- Findings later relied upon by police
Advocate Siddharth Nair ensures procedural fairness and evidentiary discipline in council proceedings to prevent criminal spillover.
F. Drugs and Cosmetics Act, 1940 & Rules, 1945
- Section 18 – Prohibited manufacture/sale
- Section 27 – Penal consequences
- Section 34 – Offences by companies
- Schedule H / H1 / X violations
G. Allied Regulatory Laws
- Clinical Establishments Act, 2010
- Biomedical Waste Management Rules, 2016
- IT Act, 2000 (electronic medical records)
- Indian Evidence Act, 1872 (expert evidence)
5. Leading Judicial Principles Governing Medical Negligence
Advocate Siddharth Nair’s litigation strategy is anchored in Supreme Court jurisprudence, including:
- Jacob Mathew v. State of Punjab (2005) – Criminal liability requires gross negligence
- Kusum Sharma v. Batra Hospital (2010) – Structured test for medical negligence
- Martin F. D’Souza v. Mohd. Ishfaq (2009) – Expert opinion mandatory before prosecution
These principles are applied consistently across High Courts including Delhi, Bombay, Madras, Kerala, Punjab & Haryana, Allahabad, Rajasthan, Madhya Pradesh, and Calcutta.
6. Investigative & Regulatory Authorities Commonly Involved
- Local Police & District Crime Units
- State CID
- Central Bureau of Investigation (CBI)
- Directorate of Health Services
- Drug Controller General of India (DCGI)
- State Drug Control Departments
- National Medical Commission
- State Medical Councils
- Nursing & Pharmacy Councils
- Consumer Dispute Redressal Commissions
- Pollution Control Boards
- Vigilance & Anti-Corruption Agencies
Managing multi-agency exposure is a core strength of Advocate Siddharth Nair’s practice.
7. Legal, Societal & Moral Challenges Faced by Medical Accused
Legal Challenges
- Presumption of guilt after patient death
- Arrest-centric policing
- Biased or non-specialist medical boards
- Overlapping jurisdictions
Societal Challenges
- Media sensationalism
- Public outrage & reputational harm
- Institutional distancing by hospitals
Moral & Psychological Challenges
- Professional guilt
- Emotional trauma
- Family and career instability
Legal defence in such cases is as much about containment and resilience as courtroom advocacy.
8. Expected Timelines for Legal Resolution
- FIR quashing: 6–18 months
- Trial-stage acquittal: 4–8 years
- High Court appellate relief: 1–3 years
- Supreme Court finality: 2–5 years
Early legal intervention dramatically reduces exposure.
9. How Advocate Siddharth Nair Protects Medical Professionals
- Pre-FIR legal risk audits
- Arrest prevention & anticipatory bail
- FIR quashing petitions
- Expert medical board coordination
- Trial-level scientific defence
- Cross-examination of prosecution experts
- Regulatory defence before councils
- Appellate & constitutional remedies
His defence philosophy is strategic, evidence-centric, and jurisprudentially disciplined.
10. Assistance for Victims of Medical Malpractice
Advocate Siddharth Nair also advises genuine victims, ensuring:
- Proper legal threshold assessment
- Avoidance of frivolous criminalisation
- Correct forum selection
- Ethical accountability
- Compensation-oriented remedies
This balanced approach enhances his credibility and standing before courts.
11. Professional Reputation & Ethos
Advocate Siddharth Nair is respected for:
- Intellectual depth
- Ethical criminal defence
- Calm handling of high-stakes cases
- Deep respect for medical science
- Strategic foresight
He is widely regarded as a lawyer medical professionals approach when their liberty, licence, and life’s work are at risk.
12. Contact Details
Advocate Siddharth Nair
Criminal Defence & Medical Malpractice Lawyer
Place: New Delhi | Delhi NCR | Pan-India
Office: 434, Lower Ground Floor, Jangpura, Mathura Road, New Delhi, NCT of Delhi, India-110014
Phone: +91-9625799959
Email: mailme@nairlawchamber.com
Website: www.nairlawchamber.com
Pharma & Hospital Corporate Criminal Defence
Advocate Siddharth Nair – Leading Lawyer for Healthcare & Pharmaceutical Prosecutions in India
New Delhi | Delhi NCR | Pan-India Representation
Click Here For Doctor-Speciality Defence Guides, Patient Rights Handbook, Checklists, Flowcharts & Hospital Training Modules

1. Overview: Criminal Liability of Healthcare & Pharmaceutical Corporations in India
Hospitals, pharmaceutical companies, diagnostic chains, and healthcare corporates in India are increasingly exposed to criminal prosecution, not merely civil liability. Regulatory tightening, public scrutiny, and outcome-driven enforcement have resulted in corporate entities and senior management being arraigned as accused in cases involving patient deaths, adverse drug reactions, clinical failures, data breaches, and regulatory non-compliance.
Advocate Siddharth Nair leads a specialised corporate criminal defence practice dedicated exclusively to pharma companies, hospitals, medical institutions, and healthcare conglomerates facing:
- Criminal FIRs and prosecutions
- Regulatory investigations
- Vicarious and managerial liability
- Multi-agency enforcement actions
- Parallel civil, criminal, and regulatory exposure
His practice is built on the legal reality that corporate healthcare prosecution is not traditional criminal law, but a complex hybrid of regulatory compliance, criminal jurisprudence, medical science, and constitutional safeguards.
2. Categories of Corporate Clients Represented
A. Pharmaceutical & Life Sciences Companies
- Pharmaceutical manufacturers
- API manufacturers
- Vaccine manufacturers
- Medical device companies
- Importers & distributors
- Contract research organisations (CROs)
- Clinical trial sponsors
- Drug marketing companies
- Pharmacovigilance entities
B. Healthcare & Hospital Corporates
- Multi-speciality hospital chains
- Corporate hospitals
- Nursing home groups
- Diagnostic laboratory chains
- IVF & fertility centres
- Blood banks
- Dialysis centres
- Telemedicine platforms
- Home healthcare companies
C. Senior Management & Officers
- Managing Directors
- CEOs / COOs
- Medical Directors
- Compliance Officers
- Quality Assurance Heads
- Plant Managers
- Hospital Administrators
- Trustees & Board Members
3. Nature of Criminal Exposure for Pharma & Hospital Corporates
Corporate healthcare prosecutions typically arise from events, not intent. These include:
- Patient death or serious injury
- Adverse drug reactions (ADR)
- Alleged sub-standard or misbranded drugs
- Off-label drug use
- Clinical trial complications
- ICU or ventilator deaths
- Infection outbreaks (HAI)
- Data breaches of medical records
- Biomedical waste violations
- Alleged suppression or alteration of records
Advocate Siddharth Nair’s defence approach focuses on breaking the chain of criminal attribution, particularly where liability is being imposed mechanically or vicariously.
4. Core Criminal & Regulatory Legislations Applicable
A. Indian Penal Code, 1860 / Bharatiya Nyaya Sanhita, 2023
Common sections invoked against corporates and management:
- Section 304A IPC – Death by negligence
- Sections 337 & 338 IPC – Hurt / grievous hurt by negligent act
- Section 269 & 270 IPC – Infection spread allegations
- Section 201 IPC – Alleged destruction of records
- Section 193 IPC – False evidence / falsified documentation
- Section 120B IPC – Criminal conspiracy
- Section 34 IPC – Common intention
Defence focus: absence of mens rea, lack of direct involvement, and improper application of vicarious liability.
B. Drugs and Cosmetics Act, 1940 & Rules, 1945
Primary statute governing pharma prosecutions.
Key provisions:
- Section 18 – Manufacture/sale of sub-standard, misbranded, or spurious drugs
- Section 27 – Penal consequences
- Section 34 – Offences by companies (director & officer liability)
- Section 26A – Prohibition of drugs
- Schedule H / H1 / X violations
Advocate Siddharth Nair frequently challenges:
- Mechanical arraignment of directors
- Absence of role attribution
- Non-compliance with sampling & testing procedures
- Invalid sanction & prosecution approvals
C. National Medical Commission Act, 2019
- Hospital-level ethical violations
- Medical Director accountability
- Institutional misconduct findings
- Findings used as basis for criminal prosecution
D. Clinical Establishments (Registration & Regulation) Act, 2010
- Infrastructure & staffing deficiencies
- Emergency preparedness
- ICU & OT compliance
- Criminal penalties for violations
E. Consumer Protection Act, 2019
- Parallel civil proceedings
- Findings often misused to bolster criminal cases
- Vicarious liability of hospitals
- Product liability against pharma & device companies
F. Information Technology Act, 2000
- Electronic medical records (EMR)
- Data privacy breaches
- Telemedicine platforms
- Cyber incidents involving patient data
G. Environmental & Allied Laws
- Biomedical Waste Management Rules, 2016
- Pollution Control Act provisions
- Hazardous waste compliance
5. Investigative & Enforcement Agencies Involved
Corporate healthcare cases often involve simultaneous multi-agency action, including:
- Local Police & Economic Offences Wing (EOW)
- State CID
- Central Bureau of Investigation (CBI)
- Drug Controller General of India (DCGI)
- State Drug Control Departments
- Directorate of Health Services
- National Medical Commission
- State Medical Councils
- Consumer Commissions
- Pollution Control Boards
- Vigilance / Anti-Corruption Agencies
- Serious Fraud Investigation Office (SFIO) (in corporate cases)
Advocate Siddharth Nair’s practice focuses on centralised legal command, preventing contradictory positions across agencies.
6. Vicarious & Managerial Liability: Core Defence Philosophy
One of the most abused aspects of healthcare prosecutions is automatic arraignment of directors, trustees, and senior officers.
Key defence principles applied:
- No criminal liability without specific role attribution
- Designation ≠ criminal responsibility
- Day-to-day control must be proven
- Statutory preconditions under Section 34 D&C Act must be met
- Board members cannot be prosecuted mechanically
Courts across India have repeatedly quashed such prosecutions when challenged effectively.
7. Defence Lifecycle for Corporate Clients
Stage 1: Pre-Crisis Advisory
- Compliance audits
- Risk mapping
- SOP and documentation review
- Incident response planning
Stage 2: Investigation & FIR
- Arrest prevention for officers
- Challenge to illegal searches & seizures
- Representation during sampling & testing
- Legal supervision of statements
Stage 3: Trial & Prosecution Defence
- Discharge applications
- Quashing of FIR / charges
- Expert scientific defence
- Cross-examination of regulators & inspectors
Stage 4: Appellate & Constitutional Remedies
- High Court petitions
- Supreme Court challenges
- Stay of coercive action
- Reputation & operational continuity protection
8. Timelines & Commercial Impact
Indicative timelines:
- FIR quashing: 6–24 months
- Trial conclusion: 5–10 years
- Appellate resolution: 2–5 years
Beyond legal timelines, corporate prosecutions cause:
- Shareholder concern
- Insurance complications
- Licensing risks
- Brand erosion
- Global regulatory impact
Early legal intervention materially reduces these risks.
9. Why Advocate Siddharth Nair for Corporate Healthcare Defence
- Specialised focus on criminal law + healthcare regulation
- Proven experience with multi-agency investigations
- Deep understanding of pharma manufacturing & hospital operations
- Strategic handling of director & officer liability
- Calm, court-respected advocacy
- Pan-India litigation capability
He is frequently consulted before FIRs are registered, reflecting institutional trust.
10. Ethical Balance: Addressing Genuine Public Harm
Advocate Siddharth Nair also advises corporates on:
- Ethical remediation
- Regulatory compliance correction
- Victim compensation frameworks
- Settlement and mediation where appropriate
This ensures legal defence without moral blindness, enhancing credibility with courts and regulators.
11. Contact – Corporate Defence Consultations
Advocate Siddharth Nair
Criminal Defence Lawyer & Criminal Defence & Medical Malpractice Lawyer – Pharma & Healthcare Corporations
Place: New Delhi | Delhi NCR | Pan-India
Office: 434, Lower Ground Floor, Jangpura, Mathura Road, New Delhi, NCT of Delhi, India-110014
Phone: +91-9625799959
Email: mailme@nairlawchamber.com
Website: www.nairlawchamber.com
New Delhi | Delhi NCR | Pan-India
Practice Focus:
Pharmaceutical Prosecutions | Hospital Corporate Defence | Regulatory & Criminal Litigation
Criminal & Regulatory Compliance in Healthcare & Pharmaceuticals
A White Paper for Hospitals, Pharma Companies & Healthcare Corporates
Prepared with Reference to Indian Criminal, Regulatory & Constitutional Law
By Advocate Siddharth Nair – Criminal Defence & Healthcare Law Specialist
EXECUTIVE SUMMARY
Healthcare and pharmaceutical corporates in India operate under one of the most criminally sensitive regulatory environments in the country. Unlike other industries, adverse outcomes alone can trigger criminal prosecution, even in the absence of intent, fraud, or recklessness.
This white paper provides a structured compliance and risk-mitigation framework to help corporates:
- prevent criminal exposure
- respond effectively to investigations
- protect directors and senior management
- ensure continuity of operations
- preserve institutional credibility
It is grounded in Indian criminal jurisprudence, regulatory statutes, and judicial precedents governing medical negligence and corporate liability.
PART I: THE CRIMINALISATION OF HEALTHCARE – AN OVERVIEW
1. Why Healthcare Corporates Face Disproportionate Criminal Risk
Healthcare is uniquely exposed because:
- Patient death is legally visible and emotionally charged
- Outcomes are retrospective, but treatment decisions are prospective
- Scientific uncertainty is misunderstood as negligence
- Media narratives influence enforcement behaviour
As a result, hospitals and pharma companies often face:
- FIRs immediately after adverse events
- Arrest threats to senior officers
- Parallel proceedings across multiple forums
- Mechanical application of vicarious liability
Indian courts have repeatedly cautioned against this trend, but compliance failure or poor response strategy often allows criminal cases to survive longer than they should.
PART II: CORE LEGISLATIVE FRAMEWORK GOVERNING CORPORATE LIABILITY
2. Criminal Law Exposure
Indian Penal Code, 1860 / Bharatiya Nyaya Sanhita, 2023
Key risk sections:
- Negligent homicide (death by negligence)
- Causing hurt / grievous hurt by negligent act
- Infection-related offences
- Record tampering & false evidence
- Criminal conspiracy and common intention
Compliance insight:
Criminal liability arises not from error, but from failure to demonstrate reasonable systems, protocols, and decision-making discipline.
3. Drugs & Pharmaceuticals Regulation
Drugs and Cosmetics Act, 1940 & Rules, 1945
High-risk provisions:
- Manufacture or sale of sub-standard drugs
- Sampling, testing, and recall non-compliance
- Director and officer liability under Section 34
- Misbranding and labelling violations
Compliance insight:
Most pharma prosecutions fail due to procedural lapses by regulators, but only when companies preserve evidence and respond correctly.
4. Healthcare Establishment Regulation
Clinical Establishments Act, 2010
- Infrastructure and staffing standards
- Emergency and ICU compliance
- Registration and renewal obligations
Compliance insight:
Infrastructure non-compliance is often used to build a criminal negligence narrative, even where causation is absent.
5. Professional & Ethical Regulation
National Medical Commission Act, 2019
- Institutional ethical responsibility
- Medical Director accountability
- Ethics committee findings feeding criminal cases
Compliance insight:
Council proceedings must be handled with the same seriousness as criminal investigations.
6. Data & Environmental Regulation
- IT Act, 2000 (medical data & EMRs)
- Biomedical Waste Management Rules, 2016
- Pollution control laws
Compliance insight:
Non-clinical violations increasingly form the foundation of criminal conspiracy allegations.
PART III: CORPORATE GOVERNANCE & BOARD-LEVEL COMPLIANCE
7. Director & Officer Liability: The Real Risk Zone
Courts have repeatedly held:
- Designation alone does not create criminal liability
- Day-to-day control must be shown
- Mechanical arraignment is illegal
However, poor governance documentation allows prosecution to survive.
Board-Level Compliance Checklist
- Clearly documented delegation of duties
- Board minutes reflecting oversight, not micromanagement
- Independent compliance committees
- Regular risk reporting to the board
- Crisis-response authority defined in advance
PART IV: OPERATIONAL COMPLIANCE FOR HOSPITALS
8. Clinical Protocol Governance
Hospitals must maintain:
- Department-wise SOPs
- Updated clinical guidelines
- Emergency escalation protocols
- ICU admission and discharge criteria
Key legal principle:
Courts assess systems, not outcomes.
9. Consent, Communication & Documentation
High-risk failure areas:
- Inadequate informed consent
- Post-event record reconstruction
- Non-contemporaneous entries
Compliance mandate:
- Consent must reflect risk disclosure, not just signatures
- Records must be contemporaneous, complete, and immutable
- EMR access logs must be preserved
10. Incident & Mortality Review Systems
Hospitals should institutionalise:
- Internal mortality review committees
- Root cause analysis (RCA) frameworks
- Non-punitive internal reporting
Legal advantage:
Robust internal review demonstrates absence of recklessness, a critical criminal defence.
PART V: PHARMA & LIFE SCIENCES COMPLIANCE
11. Manufacturing & Quality Systems
Critical areas:
- Batch documentation
- Stability studies
- Deviations and CAPA records
- Recall decision-making
Compliance insight:
Most criminal cases arise from documentation gaps, not actual drug defects.
12. Pharmacovigilance & ADR Management
Companies must demonstrate:
- Prompt ADR reporting
- Causality assessment discipline
- Transparent regulator engagement
Failure here often leads to negligence narratives in criminal complaints.
13. Clinical Trials & Research
High-risk areas:
- Informed consent of subjects
- Ethics committee independence
- SAE reporting timelines
Criminal risk increases sharply when research governance is weak.
PART VI: INVESTIGATION & ENFORCEMENT RESPONSE PROTOCOLS
14. First 72 Hours After an Adverse Event
Critical mistakes to avoid:
- Unsupervised statements
- Record alteration
- Defensive communication with families
- Internal blame allocation
Mandatory actions:
- Legal counsel engagement
- Evidence preservation
- Single communication channel
- Incident documentation freeze
15. Handling Searches, Seizures & Sampling
- Demand statutory compliance
- Document procedural violations
- Preserve duplicate samples
- Avoid voluntary admissions
Early procedural challenges often determine the fate of the prosecution.
PART VII: MULTI-AGENCY & PARALLEL PROCEEDINGS MANAGEMENT
Healthcare corporates often face:
- Police investigation
- Drug control prosecution
- Medical council inquiry
- Consumer complaint
- Civil suits
Compliance strategy:
Adopt a single, harmonised legal narrative across all forums.
PART VIII: ETHICAL REMEDIATION & REPUTATIONAL PRESERVATION
Courts increasingly value:
- Ethical acknowledgement of harm
- Remedial action
- Patient compensation frameworks
- Process correction
Defence is strongest when paired with responsibility, not denial.
PART IX: ROLE OF SPECIALISED LEGAL COUNSEL
Why Generic Criminal Defence Fails in Healthcare
Medical and pharma prosecutions require:
- Understanding of medical science
- Regulatory procedure mastery
- Board-level advisory skills
- Crisis management capability
Advocate Siddharth Nair’s practice is designed around prevention, containment, and early termination of criminal exposure, not reactive firefighting.
CONCLUSION: COMPLIANCE AS CRIMINAL DEFENCE
In healthcare and pharmaceuticals, compliance is not merely regulatory hygiene—it is criminal defence in advance.
Institutions that invest in:
- governance clarity
- documentation discipline
- early legal intervention
- ethical response systems
are far more likely to:
- avoid FIRs
- secure early quashing
- protect directors and professionals
- preserve long-term institutional credibility
AUTHOR & CONTACT
Advocate Siddharth Nair
Criminal Defence & Healthcare Law Specialist
Pharma & Hospital Corporate Defence
New Delhi | Delhi NCR | Pan-India
(Consultation and advisory engagement details may be added for publication.)
OPTIONAL NEXT DELIVERABLES
If you wish, I can now:
- Convert this into a download-ready PDF white paper
- Create sector-specific versions (hospital-only / pharma-only)
- Draft incident-response SOPs
- Prepare board-level compliance checklists
- Add risk heat-maps & flowcharts
Tell me how you would like to proceed.
Draft a medical malpractice defence handbook
Below is a comprehensive, practitioner-grade Medical Malpractice Defence Handbook drafted as a foundational reference document.
It is structured to function as:
- a definitive defence manual for doctors, hospitals, and healthcare corporates
- an internal risk-management handbook
- a litigation and investigation survival guide
- a court-aligned medico-legal reference
The tone, depth, and structure mirror professional handbooks used by insurers, hospital groups, and senior legal teams.
THE MEDICAL MALPRACTICE DEFENCE HANDBOOK
Criminal, Regulatory & Litigation Defence for Medical Professionals & Healthcare Institutions in India
By Advocate Siddharth Nair
Criminal Defence & Healthcare Law Specialist
PART I
FOUNDATIONS OF MEDICAL MALPRACTICE DEFENCE IN INDIA
1. What Medical Malpractice Is — and Is Not
Medical malpractice, in law, is not synonymous with an adverse outcome. Indian courts have consistently held that:
- Medicine is an inexact science
- Complications are inherent in treatment
- A doctor does not guarantee a cure
- Failure of treatment does not equal negligence
Criminal liability arises only when conduct crosses into gross, reckless, or culpable negligence.
This distinction is the cornerstone of every successful defence.
2. The Criminalisation Problem in Indian Healthcare
Despite settled law, medical professionals face:
- Immediate FIRs after patient deaths
- Arrest threats without expert evaluation
- Media-driven enforcement
- Parallel proceedings across forums
This handbook exists to reverse that imbalance by equipping professionals with legal foresight and procedural discipline.
PART II
TYPES OF MEDICAL MALPRACTICE CASES & DEFENCE APPROACHES
3. Categories of Allegations
Common allegations include:
- Death due to negligent treatment
- Surgical error
- Anaesthesia-related complications
- ICU or ventilator deaths
- Wrong medication or dosage
- Diagnostic errors
- Delay in treatment
- Infection-related deaths
- Consent disputes
Each category requires a distinct defence framework, not a generic response.
4. Individual vs Institutional Liability
Individual Doctors
- Clinical judgment under uncertainty
- Decision-making autonomy
- Standard of care defence
Hospitals & Institutions
- Vicarious liability
- Infrastructure and staffing allegations
- SOP compliance
- Record management
Defence must segregate personal conduct from institutional systems wherever possible.
PART III
LEGAL FRAMEWORK GOVERNING MEDICAL MALPRACTICE
5. Criminal Law Provisions
Indian Penal Code, 1860 / Bharatiya Nyaya Sanhita, 2023
Key provisions:
- Death by negligence
- Causing hurt or grievous hurt
- Infection-related offences
- Record tampering allegations
- Criminal conspiracy
Defence focus:
- Absence of mens rea
- Lack of causation
- Failure to meet “gross negligence” threshold
6. Procedural Law: The First Line of Defence
Code of Criminal Procedure / BNSS
Critical safeguards:
- Protection from arbitrary arrest
- Mandatory notice of appearance
- Expert opinion before prosecution
- Discharge and quashing remedies
Procedural violations often collapse the prosecution before trial.
7. Civil & Quasi-Criminal Forums
- Consumer Protection Act, 2019
- National Medical Commission Act, 2019
- State Medical Councils
Key principle:
Findings in these forums must be legally contained to prevent criminal misuse.
PART IV
JUDICIAL PRINCIPLES EVERY DOCTOR MUST KNOW
8. Supreme Court Jurisprudence (Core Defence Pillars)
- Jacob Mathew v. State of Punjab (2005)
→ Criminal prosecution requires gross negligence. - Kusum Sharma v. Batra Hospital (2010)
→ Outcome failure ≠ negligence. - Martin F. D’Souza v. Mohd. Ishfaq (2009)
→ Expert opinion mandatory before prosecuting doctors.
These judgments form the constitutional shield for medical professionals.
9. Tests Applied by Courts
- Bolam Test (accepted medical practice)
- Bolitho refinement (logical defensibility)
- Causation vs correlation
- Res ipsa loquitur (limited applicability)
A defence case succeeds when these tests are applied correctly and early.
PART V
DOCUMENTATION, CONSENT & RECORD MANAGEMENT
10. Medical Records: The Single Most Important Defence Tool
Common prosecution allegations:
- Incomplete records
- Post-event alterations
- Missing consent forms
Defence Best Practices:
- Contemporaneous entries
- Legible, complete documentation
- Audit trails for EMRs
- Preservation of original records
Poor documentation defeats even the best clinical defence.
11. Informed Consent: Substance Over Form
Valid consent must include:
- Nature of procedure
- Known risks and complications
- Alternatives
- Consequences of non-treatment
Consent is not a formality; it is evidentiary armour.
PART VI
HANDLING COMPLAINTS, FIRs & INVESTIGATIONS
12. The First 48–72 Hours After an Incident
Critical mistakes:
- Making unsupervised statements
- Altering records
- Emotional engagement with complainants
- Assigning internal blame
Correct response:
- Engage legal counsel immediately
- Freeze documentation
- Preserve evidence
- Designate a single spokesperson
Early mistakes often decide the entire case.
13. Police & Investigative Interaction
Key principles:
- No obligation to volunteer opinions
- Demand expert board evaluation
- Insist on procedural compliance
- Avoid self-incriminating explanations
Doctors are witnesses to science, not suspects by default.
PART VII
TRIAL STRATEGY IN MEDICAL NEGLIGENCE CASES
14. Prosecution Weaknesses Commonly Exploited
- Non-specialist expert opinions
- Retrospective hindsight bias
- Emotional testimony replacing science
- Lack of causation proof
A successful defence scientifically dismantles the prosecution narrative.
15. Expert Evidence & Cross-Examination
Defence strategy includes:
- Challenging expert qualifications
- Exposing guideline misuse
- Highlighting alternate causes
- Demonstrating reasonable judgment
Trials are won on science + law, not sympathy.
PART VIII
REGULATORY & PROFESSIONAL PROCEEDINGS
16. Medical Council Inquiries
Risks:
- Suspension of licence
- Adverse findings feeding criminal cases
Defence strategy:
- Procedural challenge
- Jurisdictional objections
- Evidence discipline
Council proceedings must never be taken lightly.
PART IX
HOSPITAL & CORPORATE DEFENCE
17. Vicarious Liability & Management Protection
Hospitals must demonstrate:
- SOP compliance
- Adequate staffing
- Equipment readiness
- Internal review mechanisms
Senior management liability must be legally ring-fenced.
18. Multi-Agency Exposure
Hospitals may face:
- Police
- Medical councils
- Drug regulators
- Consumer forums
Defence requires a unified narrative across all forums.
PART X
TIMEFRAMES, STRESS & PROFESSIONAL SURVIVAL
19. Realistic Litigation Timelines
- FIR quashing: 6–18 months
- Trial acquittal: 4–8 years
- Appeals: 2–5 years
Knowing the timeline prevents panic-driven decisions.
20. Psychological & Ethical Dimensions
Doctors face:
- Professional guilt
- Public vilification
- Family distress
A structured legal defence restores professional dignity and mental resilience.
PART XI
ASSISTING GENUINE VICTIMS
Ethical defence acknowledges:
- Genuine negligence deserves accountability
- Criminal law is not the default remedy
- Compensation and remediation matter
Balanced advocacy strengthens credibility.
CONCLUSION
MEDICAL DEFENCE IS SCIENCE-LED LAW
Medical malpractice defence is not denial.
It is scientific explanation, procedural discipline, and constitutional protection.
Doctors who:
- document well
- respond early
- seek specialised defence
stand the strongest chance of:
- early quashing
- acquittal
- professional survival
AUTHOR & PRACTICE
Advocate Siddharth Nair
Criminal Defence & Medical Malpractice Lawyer
New Delhi | Delhi NCR | Pan-India
Advocate Siddharth Nair
Criminal Defence & Medical Malpractice Lawyer
Place: New Delhi | Delhi NCR | Pan-India
Office: 434, Lower Ground Floor, Jangpura, Mathura Road, New Delhi, NCT of Delhi, India-110014
Phone: +91-9625799959
Email: mailme@nairlawchamber.com
Website: www.nairlawchamber.com
Practice Focus:
Medical Negligence Defence | Hospital & Corporate Healthcare Defence
©2026 www.nairlawchamber.com